
|
 |
|
|---|
THE OKLAHOMA VOTERS LEAGUE
REPLY TO A FEDERALLY ELECTED OFFICIALS LETTER:
Some time back an original letter was written to an Oklahoma Federally elected official, asking for her support on the issue of Medicinal Marihuana. Who in turned sent back a polite but negative response stating why she couldn't agree with a patients right to use it. ----- We in turn then sent back yet another letter requesting where she had obtained her technical detail, from what scientific studies. The letter below thus constitutes a reply to our own original reply letter.
June 7, 2011 |
|---|

The following is our own reply to the above letter.
June 7, 2011This time it is my turn to be apologetic about long delay times, but please try to understand that unlike government narcotics officials (who are paid very well for what they do), people like me have to go out and work for a living. In addition, as Im sure you are well aware, there have been many things happening within the Medical Cannabis movement with over 20 States now choosing to end medical prohibition.
[contact Information]
Dear . . .
Thank you for continuing our correspondence about the use of marijuana for medical purposes. It is good to hear from you again, and I again offer my apology for the delay in my response.
Your letter goes on to say:
I appreciate your sharing the story of your friend's struggles with chemotherapy and related weight loss. I hope she is doing well and has completely recovered.I thank you for these kind statements, this was the third time that she had been diagnosed with Cancer. And although she was a fighter, still the loss of 60 pounds in the first three weeks of her chemotherapy did take its toll. However, I can assure you that her use of Medical Cannabis during those days did help a lot.
Your letter goes on to say:
You are right to request research regarding marijuana use for such purposes as you described, and I commend your diligence in exploring the question. I hope you will allow me to briefly address current research regarding benefits and risks of marijuana for a variety of medical purposes. As you requested, I have included endnotes showing the sources of my information.Once more I wish to thank you, you are one of the few (in fact maybe the only one) who provides the footnotes needed to locate the studies in question. However, I should point out that some of these studies are now somewhat outdated; Meaning newer studies were either not being able to confirm, -- or totally disproved the original findings altogether. Ill try to document as we go along.
Your letter goes on to say:
Certain chemicals derived from marijuana have shown some modest therapeutic benefits, including some degree of relief for neuropathic pain, nausea, appetite loss in HIV/AIDS patients, and possibly for spasticity.Thank God, if only you know how many people are in total denial believe it or not making the claim that Medical Cannabis Has No Medical Uses, none what-so-ever, etc. It is good to see that at least you agree with us that Medical Cannabis does indeed have medical uses.
Unfortunately the letter goes on to say:
However, as I mentioned in my last response, it is important to distinguish between whole marijuana and those chemical substances that are derived from it. Marijuana has a derivative called tetrahydrocannabinol (THC) that the FDA has approved to treat the nausea and vomiting caused by some cancer treatments. It can also be used to help AIDS patients avoid weight loss. . . The drug "MARINOL" contains a safer, synthetic version of the active ingredient (THC) in smoked marijuana. Marinol relieves nausea and vomiting associated with chemotherapy and can assist with loss of appetite for AIDS patients. "First, YES, it is acknowledged that the drug Marinol (generic name dronabinol), does exist, does work and has many beneficial effects. However, your own statements of-and-by themselves bring up a whole host of questions:
- If Marinol is nothing more than a synthetic version of the natural product; then whats the problem with simply making use of the natural product?
--- And this is a real issue. According to the FDA, Marijuana is listed in schedule I of the Controlled Substances Act, the most restrictive schedule. . . and FDA concur(s) . . because marijuana met the three criteria for placement in Schedule I . . (e.g., marijuana has a high potential for abuse, has no currently accepted medical use in treatment in the United States, and has a lack of accepted safety for use under medical supervision). ------ But yet Marinol (which again, everyone concurs is nothing more than a synthetic version) seems to meet all the requirements. Ms. . . . , do you not see a contradiction.
- If Marinol has FDA approval then why doesnt Natural Cannabis, also have such approval?
--- It is believed that we all know the answer to this one, because its effectively AGAINST THE LAW to do medical research on Marihuana in this country. No Medical Research, no FDA approval, its as simple as that. And in case anyone has been under a rock for a few decades, heres whats going on. ----- Back in the 1970s, Medical Cannabis was classified as a Control (Class I) Substance, putting it right on up there with Heroin, etc. Now because of its status, if you wish to do medical research, you have to get a permit from NIDA or the Office of the Drug Czar. However, assuming you're brave enough to actually do that, and wait long enough (about three years on average), eventually, you will get a NO response. And if you ask them why, they will explain to you that the Drug Czars office has a Mission Statement from congress which states that they are supposed to PREVENT the use of Marihuana AND conduct scientific studies into the NEGATIVE aspects of its use. No where does it say that they are suppose to help either PROMOTE or ALLOW scientific studies into its POSITIVE effects. END OF STORY, thus no permit can be issued; and certainly not to anyone trying to obtain FDA approval, etc.
- Of what use is a prescribe-able drug that doctors are too afraid of prescribing?
--- And dont I wish that this was a joke. Using an out of state example (I knew the doctor in question personally): The narcs told the late Dr. Todd Mykuria that one of his patients was on probation and thus undergoing mandatory drug testing. AND as Marinol acts as a masking agent for Medical Marihuana, he was TOLD NOT TO PRESCRIBE IT OR ELSE. He (being a doctor) did so anyway, and true to their word, they launched a complaint with the States medical board. He almost lost his license to practice medicine. -- And this story, for obvious reasons, was not lost on other physicians who also wish to keep their medical licenses.
- Why prescribe a drug that is unfathomablely more expensive than the natural alternative?
--- This story, although mathematical is a bit long in the telling. But we do, do a good job of explaining it on the following webpage, which I hope you do get a chance to go to.
|
THE PRICE MARINOL VS NATURAL CANNABIS |

|
- Shouldnt Medical patients themselves, be the ones (with their physicians as advisors) to make the decision for themselves, just what treatment is appropriate for them; --- NOT some law enforcement official in Washington?
--- Here the problem with this issue is that the very heart of the question is freedom. The right of the people to choose that which is best for them instead of someone up in Washington. One either is supportive of that freedom or one is not.
The letter (taken a bit out of order) goes on to say:
[with reference to Marinol] Cancer and AIDS patients do not smoke THC or nabilone. These medications are available as pills, and they require a doctor's prescription.Ms. . . ., like you, I am also concerned about SMOKING anything. Maybe its my age, I just simply come from a time when medicines come in a pill form, end of story. But in any case, Medical Cannabis IS NOT a smokable medicine, but traditionally has always been an oral medicine, meaning it too comes in a pill. Need proof, our museum has documented well over 2,000 (we are getting close to 3,000 now) Medical Cannabis medicines that before the Reefer Madness campaign, were sold openly and legally in drugstores throughout our country (and yes) including Oklahoma. Just look at some of these examples Do any of them look like something that you are going to smoke to you.
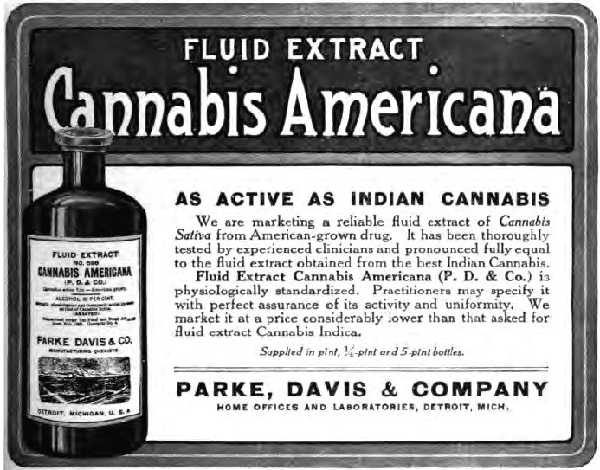
[click on image to see more examples]
You may also have noticed that some of these examples come from the Roxan Labs (which at one time was responsible for the marketing of Marinol). But the point being made here is that once relegalized (with the legal obstacles of manufacturing distribution removed), Medical Cannabis will most certainly return to its traditional roots as an oral and external medicine.
The letter also stated:
Marinol also has harmful side-effects, but its risks are known and can be supervised by a prescribing physician. Unlike smoked marijuana, doctors can also confidently prescribe dosage and indication. These statements are subject to a great deal of debate. First, all your statements (as stated above) are kind of true, but they also are kind of not.
YES, you are correct in that Marinol has harmful side-effects. In the words of one federal narcotics official, just read the warning label attached to its usage by the manufacturer, so no disagreements here.OK, so where are the problems? Essentially with just about everything thats been said; --- Lets just look at the facts.
YES, the risks known and can be (for the most part) supervised by a physician, so once again no disagreements here.
YES, unlike smoked medical marihuana, doctors can indeed prescribe dosages, etc.
The medical studies (as well as the manufacturer Marinol), all acknowledge, that due to the human digestive system, only between 10 to 20% of the active ingredient in Marinol is actually of any (medical) use. The rest being absorbed by the human body but having no medical use.
WHICH IN TURN MEANS TWO THINGS:
First that there is a 100% dosage variation. This is the equivalent of the prescribing physician handing a patient some pills and telling her to take either 8 or 16 per day, etc. Thus the wording, doctors can also confidently prescribe dosage (while true) is somewhat misleading. Its not the prescribed dosage that is important, but the dosage the patients body actually makes use of.
Second, if only 10 to 20% of the given dosage is actually seen as medicine by the human body, what happens to the other 80 to 90%? The answer is obvious and the cause of a great problem, especially for us who wish to return to the days of oral as opposed to inhaled medications. Remember, inhaled Cannabis gets into your system and takes effect almost immediately; --- Meaning you need to intake a lot less, which in turn greatly decreases those unwanted side effects.
Last of all I would like to make the following comment (without physical proof), and that is that the prescription dosages are being set NOT by medical needs, but by political ones. But again, at the present time I have no smoking gun to prove that this is so.
The letter goes on to say:
A similar derivative is called nabilone. Less injurious alternatives to medical marijuana are available through prescription for specific indications. Serostim treats wasting in AIDS patients. Megestrol acetate (Megace) is prescribed for anorexia, cachexia, and weight loss in AIDS patients. For nausea and vomiting after chemotherapy, there are other drugs to be used alone or in combination: ondansetron, metocloprainide (Reglan, and others), cortico-steriods, prochlorperazine (Compazine, and others), lorazepam (Ativan), granisetron and aprepitant (Emend).Ms. . . .. , no one over here has any medical training so all we can say is that we hope that what you are saying is correct and that those other drugs do indeed help. However, common horse sense would tell you that they are not. For example, ignoring the fact that Medical Cannabis (of and by itself) has anti-Cancer properties and focusing solely on its use as an anti-chemotherapy agent.
According to literature handed out by the federal governments own National Cancer Institute, as many as 20% (over 100,000) classified cancer deaths are actually Malnutrition-related deaths. And it must be assumed that chemotherapy treatments played no small role in that statistic. [A]
Additionally, a study just published in the Dec. 15, issue of the "Journal of Clinical Oncology," states that out of 20,000 women (cancer victims) surveyed ----only half of them actually got the full chemotherapy treatment medically called for. Reason given---the effects of the chemotherapy itself made the women so sick that the treatment had to be reduced or stopped. The study also points out that the "odds of curing breast cancer are highest when patients complete a full course of chemotherapy." OK, point being made here; --- If Marinol and ALL those other drugs are so great, then why is all that still happening?
The letter goes on to say:
Many other common claims about the benefits of smoked marijuana---treating glaucoma and seizure disorders---are discredited by the literature. Regarding glaucoma, an Institute of Medicine study observes, "Although glaucoma is one of the most frequently cited medical indications for marijuana, the data do not support this indication." [1] The study further reports there is no solid evidence smoking marijuana can treat seizures. [2]Which as you must know is a monstrously long report, put together at the behest of then Drug Czar Barry Mccaffrey, soon after the passage of Prop-215, the first State law giving medical patients the right (under state law) to use Medical Cannabis. What you might not know is that originally, it was supposed to be an actual MEDICAL RESEARCH study with actual scientific research being done, etc. However, it didnt take too long for the Drug Czar to put two and two together (meaning such research might actually lead to FDA approval) and so it was quickly changed to simply a safety study (which would not lead to FDA approval) and then mostly a research of the written literature one at that. Which, assuming you are a narc, was probably the smartest thing they could have done. Especially given the glowingly positive statements/recommendations that came out of the report. The following is taken (within context) from the Reports Ending Summary:
[1] [2]- Both references make reference to the following study: --- "The medical value of marijuana and related substances: Marijuana and medicine: Assessing the science base by Joy, J.E.; Watson, S.J.; Benson, J,A., et all
SUMMARY
Advances in cannabinoid science of the past 16 years have given rise to a wealth of new opportunities for the development of medically useful cannabinoid-based drugs.
- The accumulated data suggest a variety of indications, particularly for pain relief, antiemesis, and appetite stimulation. For patients such as those with AIDS or who are undergoing chemotherapy, and who suffer simultaneously from severe pain, nausea, and appetite loss, cannabinoid drugs might offer broad-spectrum relief not found in any other single medication.
- The data are weaker for muscle spasticity but moderately promising.
- The least promising categories are movement disorders, epilepsy, and glaucoma. Animal data are moderately supportive of a potential for cannabinoids in the treatment of movement disorders and might eventually yield stronger encouragement. The therapeutic effects of cannabinoids are most well established for THC, which is the primary psychoactive ingredient of marijuana. But it does not follow from this that smoking marijuana is good medicine.
Now granted the report is VERY, VERY negative on SMOKABLE anything and everything. However it also states the following: Until a nonsmoked rapid-onset cannabinoid drug delivery system becomes available, we acknowledge that there is no clear alternative for people suffering from chronic conditions that might be relieved by smoking marijuana, such as pain or AIDS wasting.
The letter continues:
Additionally, an American College of Physicians report notes, "For epilepsy and glaucoma, the data is much less convincing. . . .Which is true, the position paper issued by the American College of Physicians did actually say that, HOWEVER, their position paper also has glowing things to say about its medical uses just about everywhere else. For example the above quotation was taken from the following paragraph:
[3]-- Position Paper by the American College of Physicians. Entitled Supporting research into the therapeutic role of marijuana."
Preclinical and clinical research and anecdotal reports suggest numerous potential medical uses for marijuana. Unfortunately, the debate surrounding marijuana's legalization for general use has obscured scientific findings. Current available data suggest numerous indications for cannabinoids, especially antiemesis, appetite stimulation, and pain relief. For patients with AIDS or those undergoing chemotherapy, who suffer severe pain, nausea, and appetite loss, cannabinoid drugs may provide symptom relief not found in any other medication. The data supporting cannabinoid use for the relief of muscle spasticity and movement disorders is promising, but further research is needed to clarify the roles of cannabinoids in treating these conditions. For epilepsy and glaucoma, the data is much less convincing, and many of the reports supporting marijuana use for these conditions remain anecdotal. In addition, while the therapeutic effects of THC are well established, less is known about the effects and potential indications of other cannabinoids. Additional research is needed to . . . . And the quoted position paper (American College of Physicians) ends with the following:
(Ending) Conclusion:
Evidence not only supports the use of medical marijuana in certain conditions but also suggests numerous indications for cannabinoids. Additional research is needed to further clarify the therapeutic value of cannabinoids and determine optimal routes of administration. The science on medical marijuana should not be obscured or hindered by the debate surrounding the legalization of marijuana for general use.
The letter continues:
In evaluating marijuana for medical use, it is critical to also weigh any harmful side effects. High doses can induce psychosis and worsen psychotic symptoms for schizophrenic patients. There is evidence of increased rates of depression, anxiety, and suicidal thinking. [4]OooH No! You do know that you are quoting the Office of the Drug Czar; --- Not exactly the most objective nor the most truthful bunch of people out there. The following website documents just one of their golden escapades:
[4]- National Institute on Drug Abuse (NIDA), "Marijuana: Facts Parents Need to Know," available at
http://www.drugabuse.gov/marijbroch/marijparentstxt.html.
http://antiquecannabisbook.com/chap03/NCI/NCI-P1.htmMaybe it would be best to say nothing more, as we believe that the reader kind of gets the idea.
The letter continues:
Marijuana harms short -term memory and may harm patients' ability to handle complex tasks."While this statement is (kind of true), and makes for a great bumper sticker slogan, still there are a lot of problems with its technical accuracy. Yes, it appears that large dosages of Cannabis, way out of proportion to what a normal medical patient will ever need to use, do indeed effect short-term memory etc. BUT that is ONLY while that individual is heavily intoxicated. Putting it another way; -- A heavily intoxicated drunk at a bar goes around staggering all about the place. BUT as those effects ware, so does the staggering with the individual returning back to normal. Same thing can be said about Cannabis, BUT NOTE HERE, that the large amounts needed to produce this effect are WAY BEYOND what a normal patient will ever need to use. --- In other words, the statement (again while making for a good bumper sticker slogan) is essentially meaningless.
The letter continues:
Smoked cannabis has been shown to impair the ability of T-cells in the lungs' immune defense system to fight off infection and may play a role in cancer. [5]OK, got a problem, . . . now where exactly did this come from: Smoked cannabis has been shown to impair the ability of T-cells in the lungs' immune defense system to fight off infection and may play a role in cancer
[5]- Tashkin, Donald P. (2001). "Effects of Smoked Marijuana on the Lung and Its Immune Defenses: Implications for Medicinal Use in HIV-Infected Patients."
Im seeing them all over the internet -- all coming from anti-Medical Cannabis sites, but I was not able to locate it directly on the 2001 study conducted by Dr. Tashkin. [B] According to the abstract summery:
Habitual marijuana smoking may cause a number of potentially harmful effects on the lung, including the following:Which sounds very negative, but note the wording, may cause, could be etc. Meaning it wasnt the done deal all those websites were making it sound to be. But in any case Dr. Tashkin (in a later study) would go on to reverse his original statements. [C](1) acute and chronic bronchitis;The major potential pulmonary consequences of habitual marijuana use are pulmonary infection and respiratory cancer. Infectious complications could be due to smoking-related damage to the mucociliary clearance mechanism, marijuana-related impairment in the antimicrobial function of alveolar macrophages and/or fungal or bacterial contamination of marijuana. Patients with pre-existing immune deficits due to AIDS could be particularly susceptible to pulmonary infectious complications of marijuana use.
(2) extensive histopathologic alterations in the cells lining the bronchial passages that could impair mucociliary clearance or predispose to malignancy;
(3) increased accumulation of inflammatory cells (alveolar macrophages) in the lung; and
(4) impairment in the function of these important immune-effector cells, including their ability to kill microorganisms and to produce protective pro-inflammatory cytokines.
According to that studie's summary abstract: -- Donald P. Tashkin "Effects of Marijuana Smoking on the Lung", Annals of the American Thoracic Society, Vol. 10, No. 3 (2013), pp. 239-247.
ABSTRACT Regular smoking of marijuana by itself causes visible and microscopic injury to the large airways that is consistently associated with an increased likelihood of symptoms of chronic bronchitis that subside after cessation of use. On the other hand, habitual use of marijuana alone does not appear to lead to significant abnormalities in lung function when assessed either cross-sectionally or longitudinally, except for possible increases in lung volumes and modest increases in airway resistance of unclear clinical significance. Therefore, no clear link to chronic obstructive pulmonary disease has been established. Although marijuana smoke contains a number of carcinogens and cocarcinogens, findings from a limited number of well-designed epidemiological studies do not suggest an increased risk for the development of either lung or upper airway cancer from light or moderate use, although evidence is mixed concerning possible carcinogenic risks of heavy, long-term use. Although regular marijuana smoking leads to bronchial epithelial ciliary loss and impairs the microbicidal function of alveolar macrophages, evidence is inconclusive regarding possible associated risks for lower respiratory tract infection. Several case reports have implicated marijuana smoking as an etiologic factor in pneumothorax/pneumomediastinum and bullous lung disease, although evidence of a possible causal link from epidemiologic studies is lacking. In summary, the accumulated weight of evidence implies far lower risks for pulmonary complications of even regular heavy use of marijuana compared with the grave pulmonary consequences of tobacco.And to this must be added that the minor risks (if any) can be further reduced by using vaporizer inhalers and totally reduced by making use of Cannabis as an oral medicine.
The letter continues:
Smoking one cannabis joint has also been found to be as harmful as five cigarettes. Marijuana smoke has arnmonia levels 20 times higher than cigarette smoke, and hydrogen cyanide and nitrogenrelated chemicals also were more prevalent in marijuana smoke. [6]As stated above, Donald P. Tashkin "Effects of Marijuana Smoking on the Lung", [C] own research (published in the Annals of the American Thoracic Society, Vol. 10, No. 3 (2013), pp. 239-247) pretty much brings those statements into question. YES smokable Cannabis does indeed contain harmful chemicals, BUT these chemicals seem to either be negated during the smoking process or counter acted by the positive ones, etc. IN any case, unlike tobacco, they dont seem to have any harmful effects. NO PLEASE DO NOT SMOKE Historically Medical Cannabis has always been an oral medicine. And in any case smokers all seem to have bad breath. Please dont smoke.
[6]- Sarah Aldington, et a]., "Effects of cannabis on pulmonary structure, function and symptoms," Thorax Journal of Respiratory Medicine, July 3 1, 2007, available at http://thorax,bmj.com/content/62/12/1058.short.
The letter continues:
As these studies indicate, the medical evidence repudiates the notion that smoked marijuana is safe or effective.Without comment.
The letter continues:
The FDA stated, "(N)o sound scientific studies supported medical use of marijuana for treatment in the United States, and no animal or human data supported the safety or efficacy of marijuana for general medical use. There are alternative FDA-approved medications in existence for treatment of many of the proposed uses of smoked marijuana." [7]First, lets look a bit more fully at what the FDAs news release actually said: [D]
[7]- United States Food and Drug Administration, "Inter-Agency Advisory Regarding Claims That Smoked Marijuana Is a Medicine," April 20, 2006,
NEWS RELEASE
April 20, 2006 -- Last Updated: 04/08/2013
Inter-Agency Advisory Regarding Claims That Smoked Marijuana Is a Medicine
. . . Marijuana is listed in schedule I of the Controlled Substances Act (CSA), the most restrictive schedule. The Drug Enforcement Administration (DEA), which administers the CSA, continues to support that placement and FDA concurred because marijuana met the three criteria for placement in Schedule I . . . (e.g., marijuana has a high potential for abuse, has no currently accepted medical use in treatment in the United States, and has a lack of accepted safety for use under medical supervision). Furthermore, there is currently sound evidence that smoked marijuana is harmful. A past evaluation by several Department of Health and Human Services (HHS) agencies, including the Food and Drug Administration (FDA), Substance Abuse and Mental Health Services Administration and National Institute for Drug Abuse (NIDA), concluded that no sound scientific studies supported medical use of marijuana for treatment in the United States, and no animal or human data supported the safety or efficacy of marijuana for general medical use. There are alternative FDA-approved medications in existence for treatment of many of the proposed uses of smoked marijuana.
. . . . FDA has not approved smoked marijuana for any condition or disease indication. A growing number of states have passed voter referenda (or legislative actions) making smoked marijuana available for a variety of medical conditions upon a doctor's recommendation. These measures are inconsistent with efforts to ensure that medications undergo the rigorous scientific scrutiny of the FDA approval process and are proven safe and effective under the standards of the FD&C Act. Accordingly, FDA, as the federal agency responsible for reviewing the safety and efficacy of drugs, DEA as the federal agency charged with enforcing the CSA, and the Office of National Drug Control Policy, as the federal coordinator of drug control policy, do not support the use of smoked marijuana for medical purposes.
|
SEE COMPLETE NEWS RELEASE |
|
First lets look at exactly WHO IS SAYING WHAT. Direct (and very negative) quotations are being taken from:
1- Drug Enforcement Administration (DEA)
2- National Institute for Drug Abuse (NIDA), or the Drug Czars office
3- Substance Abuse and Mental Health Services Administration (SAMHSA)
(N)o sound scientific studies supported medical use of marijuana for treatment in the United States, and no animal or human data supported the safety or efficacy of marijuana for general medical use."100% correct on this one, its against the law to do medical research into Medical Cannabis in this country, so obviously there is NO scientific studies to support . . .
There are alternative FDA-approved medications in existence for treatment of many of the proposed uses of smoked marijuana."As stated elsewhere, this is not true. Even the Governments own research papers point this sad fact out.
The letter continues: "As you know, an adequate review of scientific literature is a lengthy process, and no letter can do it justice. If you would like to discuss this issue in greater detail, please feel free to write again or telephone [. . . info withheld . . .].
Actually it is we who should be thankful, it is not always that any politician (at least not at the Federal level) actually writes back in such detail. It is good that the issue is (at least) being seriously addressed after so many years of neglect. In the words of the ending summary (referencing footnotes [1],[2]); "Patients who are currently suffering from debilitating conditions unrelieved by legally available drugs, and who might find relief with smoked marijuana, will find little comfort in a promise of a better drug 10 years from now.
The letter ends with:
Thank you again for your email. Best wishes!
Sincerely,
[name /contact info withheld]
FOOTNOTES AS ENCLOSED (plus minor comments):
[1]- Joy, J.E.; Watson, S.J.; Benson, J,A., The medical value of marijuana and related substances: Marijuana and medicine: Assessing the science base. Washington, DC: National Academy Press; 1999:137-192.
http://www.nap.edu/openbook.php?record-id=6376.
[2]- Joy, J.E.; Watson, S.J.; Benson, J.A.. The medical value of marijuana and related substances: Marijuana and medicine: Assessing the science base. Washington, DC: National Academy Press; 1999:137-192.
http://www.nap.edu/openbook.php?record-id=6376.
[3]- American College of Physicians. Supporting research into the therapeutic role of marijuana.
http://www.acpontine.org/acp_news/medmarinews.htm
American College of Physicians - A Position Paper 2008
ACP strongly supports exemption from federal criminal prosecution; civil liability; or professional sanctioning, such as loss of licensure or credentialing, for physicians who prescribe or dispense medical marijuana in accordance with state law. Similarly, ACP strongly urges protection from criminal or civil penalties for patients who use medical marijuana as permitted under state laws. The research supporting THC as an effective appetite stimulant and antiemetic is abundant. In 1986, the U.S. Food and Drug Administration approved Marinol® (dronabinol), an oral synthetic form of THC, to treat severe weight loss associated with AIDS (HIV/AIDS wasting) and nausea and vomiting associated with chemotherapy for patients who fail to respond to other antiemetics.
[4]- National Institute on Drug Abuse (NIDA), "Marijuana: Facts Parents Need to Know," available at
http://www.drugabuse.gov/marijbroch/marijparentstxt.html.
[5]- Tashkin, Donald P. (2001). "Effects of Smoked Marijuana on the Lung and Its Immune Defenses: Implications for Medicinal Use in HIV-Infected Patients."
[6]- Sarah Aldington, et a]., "Effects of cannabis on pulmonary structure, function and symptoms," Thorax Journal of Respiratory Medicine, July 3 1, 2007, available at http://thorax,bmj.com/content/62/12/1058.short.
[7]- United States Food and Drug Administration, "Inter-Agency Advisory Regarding Claims That Smoked Marijuana Is a Medicine," April 20, 2006, available at
http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2006/ucmIO8643.htm
[actual correct web address is]
http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2006/ucm108643.htm
CLOSING THOUGHTS:
Once more I/we would like to thank you for your reply, I can assure you, it is more than most would have done. Of course we are saddened to hear of your viewpoint on the matter and hope that you change your mind.
As you know, although Medical cannabis was officially outlawed in the 1970s, the harassment has been going on since the creation of the Reefer Madness campaign in the 1930s. This web section documents some of Oklahomas role in the campaign and may thus be of interest to you:
http://reefermadnessmuseum.org/chap04/Oklahoma/RMOklahoma.htmIt is important to note that while this governmental dis-information campaign (era 1930s) has long ago been discredited (e.g. Note the police are no longer going around claiming that Marihuana is turning anyone into a cold blooded killer, etc.). Still it left behind a mind-set that still effects us to this very day. Some cops (et al), really believe that Medical Cannabis is a conspiracy. No, joke, they believe that the unwashed hippie, deliberately got cancer, just so hell have an excuse to use Medical Cannabis. And of course they are not fools and are not going to fall for it, etc. . . A situation which today is (thank God) finally changing as more and more people have began to open their voices and speak up.
Ms. . . . , obviously you are somewhat negative on the subject, and I dont believe that a short Rah, Rah, speech is going to change your view point. However, hope that this letter can at least cast doubt in your mind; Especially about those around you who you might have been listening to. People whose nefarious agendas (especially here in Oklahoma) must be called into question.
It is our hope, that by going over the actual facts (not what Oklahomas Bureau of Narcotics tells you, but the facts), that you will eventually change your mind on this matter. That you will eventually do the right thing.
==============
FOOTNOTES:
[A]- Nci_u6%7E1 citing references
(14) Robinson G, Goldstein M, Levine GM: Impact of nutritional status on DRG length of stay. Journal of Parenteral and Enteral Nutrition 11(1): 49-51, 1987.
(15) Reilly JJ, Hull SF, Albert N, et al.: Economic impact of malnutrition: a model system for hospitalized patients. Journal of Parenteral and Enteral Nutrition 12(4): 371-376, 1988.
[B]- Journal of Cannabis Therapeutics (2001) Vol. 1, Issue: 3/4, Pages: 87-102
http://www.mendeley.com/research/effects-smoked-marijuana-lung-immune-defenses-implications-medicinal-hiv-infected-patients/
[C]- Donald P. Tashkin "Effects of Marijuana Smoking on the Lung", Annals of the American Thoracic Society, Vol. 10, No. 3 (2013), pp. 239-247.
http://www.atsjournals.org/doi/abs/10.1513/AnnalsATS.201212-127FR?prevSearch=marijuana&searchHistoryKey=
[D]- Actual copy can be found at
http://www.fda.gov/NewsEvents/Testimony/ucm114741.htm

|
-- BACK -- MORE REPLY LETTERS |
WANT TO KNOW MORE:
=====================
Due to space / download time considerations, only selected materials are displayed. If you would like to obtain more information, feel free to contact the museum. All our material is available (at cost) on CD-Rom format.
CONTACT PAGE
(A Pro Medical cannabis Organization)
ADD YOURSELF TO OUR MAILING LIST:
http://drugsense.org/lists/listform.htm?okvotersleague
|
BACK TO OKLAHOMA MAIN PAGE |
|
Our Motto - We're pro-Medical Cannabis and we Vote!